
Some clients are concerned for cosmetic reasons, as these nodules range from rather unsightly to complete eyesores. Others are concerned that these growths may be cancerous.
Sebaceous is a Latin word relating to a sebaceous gland or its secretion. Hyperplasia originates from ancient Greek words “huper,” meaning “over,” and “plasis,” meaning “formation.” Thus, hyperplasia is an increased amount of organic tissue that results from cell proliferation.
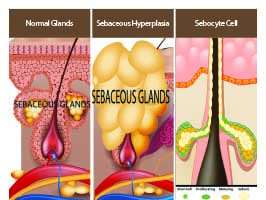
Sebaceous hyperplasia or sebaceous gland hyperplasia is defined as a common, benign condition of enlarged sebaceous glands holding trapped sebum, presenting in middle-aged and senior adults. Hyperplasias are classified as benign tumors. Simply put, a sebaceous hyperplasia is a giant oil gland protruding through the surface of the skin with tissue that has formed a harmless tumor.
 RISK FACTORS
RISK FACTORS
There are a variety of risk factors in individuals that are related to developing sebaceous hyperplasia. For instance, adults over 40 that have oily or combination skin types; light-skinned individuals with excessive sun exposure (ultraviolet radiation damages skin cells and oil glands); and patients with Muir-Torre syndrome are all at high risk. Additionally, it is common among kidney transplant patients or anyone taking the immunosuppressant medication cyclosporine. Cyclosporine also treats Chron’s disease, psoriasis, rheumatoid arthritis, nephrotic syndrome, and chronic dry eye. Genetics can also play a role. If parents or other family members have the condition, a person’s risk level is elevated. Also, oily skinned rosacea patients appear to have a higher occurrence of this condition.
RECOGNIZING THE CONDITION
Most sebaceous glands are found on the face, neck, and chest; other locations include the back, shoulders, upper arms, breast, the groin area, and armpits.
Lesions present as small, pale, asymptomatic, soft, yellowish papules, sometimes with a smooth surface and other times appearing lumpy.
These bumps typically measure from one to five millimeters, with most averaging from two to three millimeters. Clients may have one or multiple lesions on the face, particularly the nose, cheeks, and forehead.
Sebaceous hyperplasias can become red, irritated, and even bleed after scratching, shaving, or other forms of trauma.
Occasionally, a small amount of sebum can be extracted from a central, nave-like depression in the nodule which often leads a client into thinking that this is an acneic breakout. The depression in the center of the nodule signifies sebaceous hyperplasia.
VARIANTS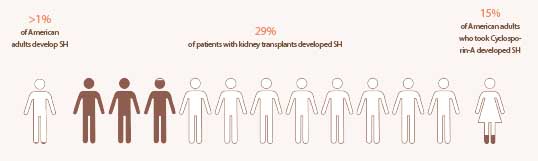
This condition takes on a few interesting forms (variants) that a medical provider may diagnose.
Giant Senile: There is a reported case of a 75-year-old, Japanese male with a dome-shaped, skin-colored nodule on his right cheek. The lesion was 10 millimeters in diameter and had multiple, small, pitted depressions on its surface. Imagine a nodule almost half an inch in diameter with numerous craters!
Linear: These are multiple hyperplasias forming a straight line.
Nevoid presentations resemble a nevus – a malformation of skin due to pigment or capillaries that are raised or flat.
Zosteriform Arrangement nodules follow a linear pattern similar to shingles.
Juxtaclavicular presents as small papules arranged in parallel rows along the clavicle bone that look like a string of pearls.
Diffuse nodules spread out over a defined area.
Familial (premature) – reported cases in children suggest that genetics may play a role.
Multiple eruptions occur before or by puberty and progress as the child ages.
CONFIRMING DIAGNOSIS
Professionals only analyze the skin; to get the correct diagnosis, the client must see a medical provider who uses the following steps to confirm findings, discover the cause, and choose the best treatment option for the patient.
STEP 1
Physical Examination

STEP 2
Medical History Assessment
STEP 3
DermoscopyDermoscopyLesion Analysis

STEP 4
Skin AnalysisSkin AnalysisWood Lamp

STEP 5
Skin Biopsy

UNDERSTANDING THE CONDITION
The exact etiology is unknown; however, several studies point towards relevant theories.
Contributing Factors
One contributing factor of sebaceous hyperplasia is the decrease in androgen levels associated with aging.
Ultraviolet radiation is not a cause, only a cofactor, as hyperplasias also present on body areas not exposed to sunlight, including the buccal mucosa (inner lining of the cheeks and back of the lips), areola, vulva, and penis.
There may be a genetic connection, although more studies are needed to support this theory.
A weak immune system; long-term immunosuppression in post-renal transplantation patients taking cyclosporin-A has led to the development of sebaceous hyperplasias.
How and Why Sebaceous Hyperplasia Develops
Sebaceous glands are a part of the pilosebaceous unit found in the dermis. They are located throughout the body except for palms and the bottom of feet. The largest and most prevalent sebaceous glands are located on the face, chest, back, and upper arms. Sebaceous glands secrete an oily, waxy substance consisting of fats and cellular debris, called sebum, that lubricates the surface of the skin.
During late stages of gestation, the sebaceous glands are large and produce vernix (the waxy white substance) coating the skin of newborn babies. After birth, the size and activity of the glands regress due to the waning of the mother’s hormones. The glands remain small until puberty. The number of sebaceous glands remains constant throughout life, but their size and activity levels are influenced by age and hormones, as they are sensitive to androgen hormones. The glands enlarge due to androgen dominance which causes an increase in oil production. By the 30s, sebaceous glands have reached their maximum size.
Sebocytes are the cells that compose the sebaceous unit and produce sebum. Sebocytes in normal sebaceous glands differ from those affected by decreased androgen levels that cause sebaceous hyperplasia. Sebaceous hyperplasia sebocytes are smaller, with larger nuclei, that produce less sebum and migrate slowly through the gland. As this slowing occurs, the gland enlarges with a widened duct and a high number of basal cells.
With age, androgen levels decline and sebocyte turnover decreases causing a buildup of sebocytes. This stockpile of cells causes the sebaceous gland to enlarge, creating a benign tumor-like growth. Think of acne, where sebum forms a plug to clog a pore. There is a blockage with sebaceous hyperplasia, as well, but the gland does not recognize this, so it continues to produce more sebum and to enlarge. They can inflate up to ten times their normal size becoming a cosmetic eyesore on the face, neck, or chest.
SEBOCYTE METABOLISM
Sebocytes contain androgen-metabolizing enzymes, including: 5-alpha-reductase type I, 3-beta-hydroxysteroid dehydrogenase, and 17-beta-hydroxysteroid dehydrogenase type II.
These enzymes metabolize dehydroepiandrosterone-sulfate into dihydrotestosterone (DHT).
Next, dihydrotestosterone binds to receptors attached to the sebocytes, causing an increase in the size and metabolic rate of the sebaceous gland.
Studies have shown elevated levels of 5-alpha-reductase activity in the scalp and facial skin, enabling testosterone and dihydrotestosterone to stimulate more sebaceous gland proliferation in these areas.
 If estrogen were the dominant hormonal influence, the skin would experience a decrease in sebaceous gland secretion.
If estrogen were the dominant hormonal influence, the skin would experience a decrease in sebaceous gland secretion.
PREVENTION
Because there is not a definitive cause for sebaceous hyperplasia, a prevention plan that will be 100 percent effective cannot be determined. The best way to avoid developing this condition is by maintaining a healthy diet, lifestyle, and skin care routine. Clients should be sure to include the following:
- Daily cleansing, morning and night.
- Regular exfoliation, including professional facial peels.
- Daily intake of vitamins and minerals.
- Avoidance of foods that interfere with hormone or pH levels. Limited consumption of red meats, cheese, and butter. Organic milk, organic fresh foods rich in vitamin C, beta-carotene, the omegas, and probiotics should be prioritized.
- Drinking adequate amounts of water. The National Academy of Medicine (NAM) updated recommended guidelines to 3.7 liters for an adult male and 2.7 liters for a female, but these numbers include the water found in foods eaten. People should drink when thirsty and, when drinking caffeinated beverages, make a concentrated effort to drink additional amounts of water.
- Areas affected by sebaceous hyperplasia should not be irritated.
- Regular exercise promoting proper circulation to skin, keeping it vibrant and healthy.
- Attention should be paid to suspicious lesions; if something does not look right, clients should see a medical professional.
TREATMENT OPTIONS
There are numerous treatment options available to the client. First, the client must decide if they plan to manage the condition or would prefer to eradicate it; keeping in mind that, although one or many hyperplasias may be removed, new ones can develop at any time. The client should also consider the possibility of developing post-inflammatory pigmentation or having a depressed scar with medical removal methods.
 MANAGING HYPERPLASIA WITH HOMECARE AND OVER-THE-COUNTER PRODUCTS
MANAGING HYPERPLASIA WITH HOMECARE AND OVER-THE-COUNTER PRODUCTS
There are many home remedies for addressing sebaceous hyperplasia available to the client.
Salicylic Acid
This beta hydroxy’s keratolytic action cleans the surface and penetrates deep into the pore, infiltrating the oil buildup to unclog impactions. Its anti-inflammatory benefits help diminish the appearance of the nodules.
Citrus Limonum (Lemon) Juice or Oil
Lemon oil is a potent essential oil that attacks sebaceous hyperplasia with its antiseptic and astringent properties.
Lemon oil also balances the pH of skin. Use caution around the eyes due to its acidity.
Retinol
Vitamin A-based solutions, like retinol, have delivered positive effects on sebaceous hyperplasia, as they temporarily shrink oil glands.
Malic and Acetic Acids (Apple Cider Vinegar)
Vinegar balances the pH of the skin while dissolving the lesions and inhibiting their redevelopment. Malic acid (found in apples) is an alpha hydroxy acid that has hydrating, exfoliating, and pH-balancing properties.
Mentha Piperita (Peppermint) Oil
This essential oil is an antiseptic, antibacterial, and astringent that absorbs into the skin, eliminating excess oil responsible for papules. Its anti-inflammatory properties assist in returning the glands to their normal size.
Malic and Acetic Acids (Apple Cider Vinegar) with Mentha Piperita (Peppermint) Oil
Blending these three ingredients gives the benefits of an antioxidant and anti-inflammatory with the keratolytic action of vinegar.
Mentha (Mint) Juice
Mint juice works in a comparable way to peppermint oil. Clients can apply natural mint juice directly to the overgrowths at night, leave on, then wash off with warm water in the morning.
Mentha (Mint) Juice and Curcuma Longa
(Turmeric) Powder
Turmeric (curcuma longa) provides antitumor, anti-inflammatory, and anti-bacterial benefits, along with its component curcumin being anti-inflammatory. Mint juice is cooling, an excellent cleanser, antipruritic, and an astringent. Clients can mix mint juice and turmeric powder into a paste, apply to the nodule, and leave on for five to twenty minutes before washing off with warm water.
Trifolium Pratense (Red Clover) Extract
Phytoestrogen isoflavones (plant compounds with estrogenic activity) can help suppress sebaceous hyperplasia due to their estrogen hormone influence. Biochanin A, derived from red clover extract, works by suppressing (types 1 and 2) 5-alpha reductase, thereby reducing sebum production. It also improves the desquamation process and increases the skin’s contraction properties. Clients should consider preparing it as a tea and drinking twice daily.
Hamamelis Virginiana (Witch Hazel)
This is a potent astringent rich in tannins. Tannins tighten pores and control oil secretions. To use, clients can apply one to two drops of witch hazel oil to the affected
area daily.
Suggested Application
To apply the above topical treatments, clients should gently dab a cotton swab directly on the affected area each night for a week or until the lesion disappears. If there is no change, they should discontinue use and see a clinician or medical provider for other options.
 TEMPORARY OR PERMANENT ERADICATION IN THE SPA OR PHYSICIAN’S OFFICE
TEMPORARY OR PERMANENT ERADICATION IN THE SPA OR PHYSICIAN’S OFFICE
Clients can diminish or choose temporary or permanent eradication of sebaceous hyperplasias. Keep in mind that, if not entirely removed, the affected glands will produce new hyperplasias. Additionally, new hyperplasias can develop in surrounding follicles.Maintenance treatments are required to keep the condition in check.
Medical providers may recommend the following treatments; however, it is the individual’s decision as to which option best meets their needs.
Chemical peels using salicylic, bichloroacetic (BCA), also known as dichloroacetic (DCA), or trichloroacetic (TCA) acids blanch lesions, destroying the tissue. The permanency of this choice depends on the percentage of the acid used, as the complete destruction of the gland is necessary to become a permanent fix.
Surgical removal (excision) is a complete removal that may result in scarring, without risk of reoccurrence.
Photodynamic therapy is a light-emitting therapy. Skin is pre-treated using a photosensitizing, prescription gel (5-aminolevulinic acid (ALA), that reacts with the light source, either IPL or a 405-420 nanometer blue light laser. This option is a multi-visit treatment.
Anti-androgen medication: Reducing testosterone levels decreases sebum production from the oil glands. Anti-androgen therapy works by blocking and reducing the production of androgen (male) hormones.
Electrocauterization: An electrically charged needle vaporizes the nodule. A scab forms that falls off in a few days. It can cause post-inflammatory hyperpigmentation in the treated area. Electrocauterization provides 100 percent removal, but there is no guarantee that another lesion will not develop nearby.
Laser therapy: A technician uses a diode, pulsed dye (PDL), or erbium laser to smooth the surface of skin and remove the trapped sebum.
Cryotherapy: Nodules are frozen with liquid nitrogen, causing them to fall off. This option also carries the risk of developing post-inflammatory hyperpigmentation.
Prescription retinoids are available as an option that temporarily shrinks sebaceous glands, but sebaceous hyperplasia returns after discontinuing therapy.
Radio Frequency (RF): A number of treatments that use radio frequency technology are used to treat sebaceous hyperplasia. Some of these treatments involve heating the sebum or transmitting a high-frequency current to vaporize the lesions. In some treatments, new hyperplasias can appear, though treated ones do not typically return.
IPL: A series of IPL procedures can address small nodules and be helpful for surrounding redness. Multiple treatments may be required but can be a good option for sensitive, fair-skinned individuals.
As professionals are armed with the most current knowledge, clients do not have to endure these ugly growths any longer. They can choose which direction works best for them to achieve healthy, beautiful skin.
References
1 Boschnakow, A., T. May, C. Assaf, B. Tebbe, and Chc Zouboulis. “Ciclosporin A-Induced
Sebaceous Gland Hyperplasia.” The British Journal of Dermatology 149, no. 1 (July 2003):
198-200.
2 Salim, A., S.M. Reece, A.G. Smith, D. Harrison, H.M. Ramsay, P.N. Harden, A.A. Fryer.
“Sebaceous Hyperplasia and Skin Cancer in Patients Undergoing Renal Transplant.” Journal
of the American Academy of Dermatology 55, no. 5 (Nov 2006): 878-881
3 Johnson P.J. and F. Heckler. “Muir-Torre Syondrome.” Annals of Plastic Surgery 40, no. 6 (June 1998): 676-677
4 “Understanding Sebaceous Hyperplasia.” Healthline. https://www.healthline.com/health/skin-lumps/sebaceous-hyperplasia.
5 “Radiosurgery.” Dermacare Medical PC. http://www.dermacaremedical.com/radiosurgery.php.
6 Bailey, Cynthia, M.D. “Dermatologist Tips to Treat Sebaceous Hyperplasia.” Dr. Cynthia
Bailey Skin Care. September 5, 2012. https://www.drbaileyskincare.com/info/blog/dermatologist-tips-to-treat-sebaceous hyperplasia.
7 Fritsch, Martin, Constantin E. Orfanos, and Christos C. Zouboulis. “Sebocytes Are the Key Regulators of Androgen Homeostasis in Human Skin.” Journal of Investigative Dermatology 116, no. 5 (May 2001): 793-800. doi:10.1046/j.1523-1747.2001.01312.x.
 Brenda Linday is a licensed aesthetician, licensed aesthetic instructor, and certified aesthetic consultant with over 12 years of experience in the medical aesthetic industry. She offers consulting services to medical and aesthetic companies desiring to build strong sales and education teams. She also develops educational and engagement-marketing content for employees, contractors, practitioners, and industry distributors around the world. Linday’s passion is to share her wealth of knowledge with other like-minded professionals who believe that education is key to building lasting relationships with clients, making each clinician more successful by increasing client satisfaction.
Brenda Linday is a licensed aesthetician, licensed aesthetic instructor, and certified aesthetic consultant with over 12 years of experience in the medical aesthetic industry. She offers consulting services to medical and aesthetic companies desiring to build strong sales and education teams. She also develops educational and engagement-marketing content for employees, contractors, practitioners, and industry distributors around the world. Linday’s passion is to share her wealth of knowledge with other like-minded professionals who believe that education is key to building lasting relationships with clients, making each clinician more successful by increasing client satisfaction.