SKIN OF COLOR PHYSIOLOGY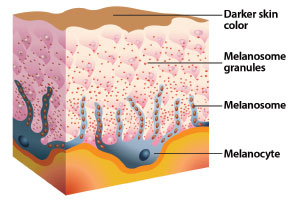
One of the main differences with dark skin types in comparison with lighter skin types is that there are varying degrees of pigmentation seen in the multicultural population. While everyone is born with the same number of pigment-producing melanocyte cells, in darker skin colors, the melanosomes within the melanocyte cells are a different shape and produce melanin in greater quantities.
Melanosomes are where the synthesis of melanin takes place via the enzyme tyrosinase, the key enzyme that sets melanin production in motion. There are two forms of melanin produced by melanosomes: pheomelanin, which is red-to-yellow in color, and eumelanin, which is dark brown-to-black.
One of the most important things to know when administering exfoliation procedures for ethnic clients is that the reason they demonstrate less pronounced photosigns of aging in comparison to Caucasian clients is largely due to the photoprotective effects of melanin. However, it is that same photoprotective response that creates pigmentation disorders in ethnic skin and is why it is critical to properly select the right exfoliation method and/or solution for ethnic clients.
The good news is that there are a wide range of excellent cosmetic exfoliation procedures that are safe and effective for darker skin types. Of course, a satisfactory outcome will start with an expert skin analysis and lifestyle consultation. From there, professionals will have the knowledge they need to select the appropriate exfoliation solution for their clients.
SKIN PEELS
The epidermis is composed of multiple layers of epidermal cells. These cells provide a barrier against the environment, protecting deeper, more delicate tissues. They also help maintain an even internal temperature, preventing dehydration. Epidermal cells are anchored together by microscopic fibers called tonofilaments, which run between individual cells. An extracellular lipid surrounds each cell, acting as a sort of glue to further keep cells together. Over time, these cells are invisibly shed through the body's natural means of exfoliation. Speeding up this process with an exfoliation procedure not only restores a more youthful glow to the skin, but also addresses other unwanted signs of the aging process.
The difference between microdermabrasion and peeling solutions is that mechanical exfoliation breaks tonofilaments, while liquid peel solutions work to dissolve the lipids that bond cells together. Skin care professionals must guide their client to the most appropriate type and level of peel to address their concerns. They must also set realistic expectations for their healthy skin goals.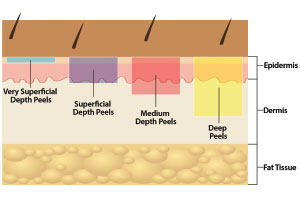
REALISTIC EXFOLIATION
The selection of an active peeling solution should be based on the desired degree of skin rejuvenation. If the client's skin concerns are predominantly superficial, then a mild enzyme or low-concentration enzyme or acid peel is appropriate. However, if the client is presenting problematic skin conditions, then deeper peels will be necessary to resolve and restore the skin's health and beauty.
Deeper peels formulated with higher concentrations of acids blended for increased penetration and results carry with them the potential for complications, making them riskier to use in skin of color, especially if the professional has not pre-conditioned the skin to reduce the risk of abnormal pigment development. These peels are usually referred to as chemical peels, work much deeper in the epidermis, and also have benefits into the dermal layer of the skin. While milder peels are performed with frequency, chemical peels are performed less frequently to allow for complete healing and skin rejuvenation to take place below the epidermis.
Educating clients about the potential side effects of skin-rejuvenating peels – like redness, irritation, dryness, flacking, and peeling – should be part of the discussion prior to the peel, as well as setting realistic goals and expectations. Realistic goals of skin peels may include reducing mild scarring, softening fine lines and deep wrinkles, evening the skin tone, and reducing excessive sebum. Other goals include dissolving stubborn blackheads, preventing the reoccurrence of acne breakouts, and softening the appearance of scarring and stretch marks. Unrealistic goals of skin peels include removing disorganized cells, like moles on the skin; changing pore diameter or removing pore openings; removing or improving keloid-type scars; removing broken capillaries; and lifting deep wrinkles.
THE FOUR LEVELS OF SKIN PEEL DEPTH
Peel formula's ingredients, concentration, and pH play a large role in determining the ultimate depth of a peel. Other variables, such as whether a pre-peel degreasing step is performed, the layers of solution applied, and the length of time the peel is allowed to stay on the skin, can also make a difference. Professionals should be aware that no matter what type or depth of peel is used, exfoliation always increases a person's sun sensitivity. Always recommend that clients wear a broad spectrum SPF of 15 or higher when using any type of chemical or physical exfoliation.
Very Superficial Depth Peels
These peels are more of an exfoliation using skin brushing, polishing agents, enzymes, and low concentrations of alpha hydroxy acid (10 percent or below) and beta hydroxy acid (three percent or below). The most superficial layers of the stratum corneum are softened and removed or thinned during the exfoliation process. This level of peel is recommended to begin the process of skin conditioning for deeper peels in skin of color.
Superficial Depth Peels
This type of peel removes the epidermal cell layers to a greater degree than a very superficial depth peel, but is still considered a refreshing form of a skin peel or a lunchtime peel.
They help with reducing the appearance of uneven, mildly blotchy skin discoloration and remnant acne discoloration. They also help to decongest pores and resolve mild cases of acne breakouts. These peels are formulated with concentrations of 15 to 30 percent alpha hydroxy acid and five to 20 percent beta hydroxy acid and are the most common forms of peeling solution for clients of all skin colors. This level of peel is recommended once two or three very superficial peels have been performed to learn how the client's skin responds to skin exfoliation. In most cases, many problematic skin conditions can be resolved at this level with little-to-no risk of peel complications. Usually, a series of peels performed every other week will be needed for optimal results.
Medium Depth Peels
These peels penetrate to the basement of the epidermis and have the potential for greater correction for problematic skin conditions. A medium depth peel, such as a seven to 14 percent Jessner's Solution and 10 to 20 percent trichloroacetic acid peel, is far more likely to be associated with potential complications. Inflammation from this level of peel may temporarily produce an increase in skin discoloration. Medium peels are only appropriate for people with darker skin tones if the skin has been properly conditioned with tyrosinase inhibitors, such as hydroquinone, kojic acid, ascorbic acid, chromanyl palmitate, and sunscreen 30 to 90 days prior to the peel, due to the risk of irregular pigmentation following the procedure. This level of peeling solution should only be recommended for ethnic clients after they have successfully tolerated the superficial level of exfoliating solutions without complications and if they are compliant to the homecare regimen.
Deep Peels
Deep peels penetrate through the epidermis to the papillary dermis depending on the procedure used. These peels are usually performed with 35 percent trichloroacetic acid and phenol. They are not normally procedures that an aesthetician would administer, nor are they ideal for Fitzpatrick skin types III through VI because of their skin-bleaching effect. Another risk to consider with deep peels for darker skin colors is post-inflammatory hyperpigmentation. Professionals should only refer their clients to a physician for a deep peel if the degree of correction has not been achieved with the superficial and medium depth peels and the client is seeking greater results and is willing to accept the risks associated with this level of skin exfoliation.
Exfoliating peels can truly retexturize the skin and restore radiance and a youthful appearance with minimal complications. Additionally, skin peeling procedures have been studied and tested by many physicians and skin care professionals and have been proven to be a safe, non-invasive method for effective skin rejuvenation in most ethnic skin types.
 IDEAL EXFOLIATING PEELS FOR ETHNIC SKIN
IDEAL EXFOLIATING PEELS FOR ETHNIC SKIN
Enzyme Peels
Enzyme peels are known for treating clients with sensitive skin and those who are sensitive to alpha hydroxy acid and beta hydroxy acid peels. Enzyme peels loosen and remove dead skin cells, cleanse pores, and improve skin tone and texture with minimal-to-no downtime or adverse skin irritation. Natural enzyme peels are safe for all skin types and do not wound the skin. Popular ingredients for enzyme peels include papain from papaya, bromelain from pineapple, pumpkin; blueberry; and pancreatin, a biological.
Alpha Hydroxy Peels
Glycolic acid peels are the most commonly used alpha hydroxy acid peels and are known for being an ideal resurfacing agent for a wide variety of skin types. Glycolic works by dissolving the intercellular lipids that hold dead cells to the skin's surface. Out of this group of acids, glycolic acid is the most useful for cosmetic treatments because of its small molecular structure, which allows for greater penetration. Factors that determine whether alpha hydroxy acid peels result in desquamation include the concentration of the acid, the pH of the formulation, the amount of acid delivered to the skin, the frequency of use, and, most importantly, the duration of time the acid is left on the skin. There have been ample studies showing the successful use of glycolic acid for treating melasma, hyperpigmentation disorders, photodamage, and acne in ethnic skin.
Lactic acid, which is also an alpha hydroxy acid, acts similarly to glycolic acid and is also a safe and effective peeling agent for darker skin types. While it works in much the same way as glycolic acid, it does not have the same dehydrating effects because its molecules are larger, so it is less permeable and milder on the skin. It is also a natural humectant, which is why it is considered to be an excellent exfoliant for dry, sensitive skin.
Beta Hydroxy Peels
Salicylic acid, a beta hydroxy acid traditionally used for treating acneic skin conditions, is an excellent peeling agent for numerous conditions in dark skinned individuals, including acne, melasma, and post-inflammatory hyperpigmentation. It has a pigment-diffusing effect on the skin and is an adequate comedolytic agent due to its antibacterial benefit. Its mechanism of action in decreasing pigmentation is slightly different from that of glycolic acid. Salicylic acid is anti-inflammatory and, as a result, serves to decrease the post-inflammation hyperpigmentation that could potentially follow the use of peeling agents on ethnic skin.
Jessner's Solution
Jessner's Solution has been in use as a peeling agent for decades. This combination of seven to 14 percent resorcinol, salicylic acid, and lactic acid in an ethanol base has been extensively utilized as an exfoliating peel for all skin types. Jessner's Solution produces keratolysis and protein coagulation, removing the stratum corneum and kerato-coagulating portions of the epidermis. The three keratolytic agents used together create a synergistic effect for problematic skin conditions; a big advantage of the Jessner's Solution is that it contains resorcinol, a phenolic skin lightening agent. It has been well documented that Jessner's Solution is well-tolerated in Fitzpatrick skin types III through VI. The application of Jessner's peel may be light or heavy, depending on the number of layers applied, which will be determined by the clinical appearance of the skin and individual tolerance. The Jessner's Solution peel may be repeated at two-to-four month intervals, depending on the client's skin-rejuvenation goals.
Trichloroacetic Acid Peel
Although commonly used in lighter skin types, trichloroacetic acid (below 35 percent) is frequently used in darker skin types when the skin has been properly pre-conditioned with tyrosinase inhibitors and sunscreen. These peels are very effective for pigment dyschromia and are considered to be the gold standard of peeling agents. This acid can be used to treat a wide range of ethnic clients with age-related skin conditions, like pigment disorders; photoaged skin; light-to-deep wrinkles; acne scarring; and thick, uneven skin tone and texture. Before administering this peel to any client, recommend a pre-treatment regimen of exfoliating agents, such as retinoids, retinols, glycolic acid, and pigment-suppressing agents (tyrosinase inhibitors) applied for 30 to 120 days prior to the actual peel procedure. This regimen will help the peeling agent penetrate more evenly, aid in rapid recovery, and reduce the risk of complications.
PRECAUTIONS
There are many precautions a professional should take with ethnic clients when it comes to superficial peels, including a history of herpes simplex virus (cold sores); previous chemical- or mechanical-resurfacing procedures; a history of topical medication use, including retinoids and antibiotics; and a history of oral medication use, including Accutane, minocycline, and erythromycin. Professionals should also avoid raised moles, skin tags, keloids, and scars less than six months old and permanent makeup. Furthermore, they should be aware of the client's current skin care regimen, physical and mental health, and expectations.
There are also contraindications for ethnic clients with medium peels, including any type of dermatitis, such as eczema, psoriasis, and seborrhea; viral lesions, including herpes simplex virus, impetigo, and warts; opened or unidentified skin lesions; and tattoos and permanent makeup. Moreover, professionals should be aware of clients who are exposed to sunlight on a regular basis; autoimmune disorders, such as HIV/AIDS, hepatitis C, lupus, and vitiligo; clients with skin cancer or those receiving radiation or chemotherapy; clients taking oral anticoagulants; clients using photosensitive medications; clients who are pregnant or breast feeding; and clients with heart problems.
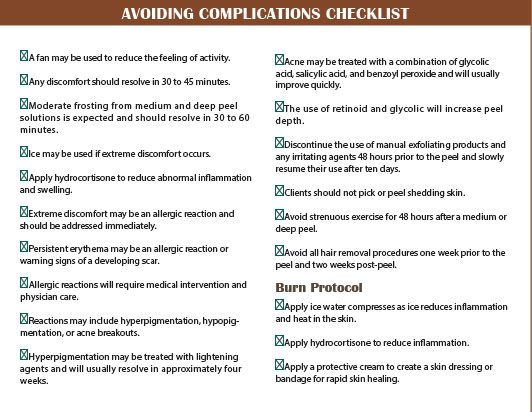
POTENTIAL PEEL COMPLICATIONS
Rejuvenating the skin with peeling solutions that are essentially wounding agents can produce dramatic visible improvements for most ethnic individuals without worry of side effects or complications. However, thorough knowledge of the agent being used and its effects on the selected skin type and condition being treated is critical to avoiding complications. Complications do occur and the potential for unwanted side effects increases depending on the peel agent and depth of wounding.
Post-Inflammatory Hyperpigmentation
Superficial peel complications are usually only transient pigmentary reactions. Post-inflammatory hyperpigmentation is rare, but can be triggered by sun exposure after the peel. In some cases, hyperpigmentation may develop as soon as four or five days post-procedure from the inflammatory response induced from the trauma of the peel. It usually resolves on its own without the use of topical treatment, but this condition responds well to topical lightening agents.
Post-Inflammatory Hypopigmentation
Post-inflammatory hypopigmentation is usually associated with deep peels, but it can occur with lighter peels as well. Any peel that causes exfoliation will lighten the skin because melanin is dispersed throughout the epidermis. If professionals shed skin cells containing melanin, the skin will appear lighter. However, the lightening effect is temporary as new melanin is continually being formed. As the level of the peel gets deeper, the degree of lightening or hypopigmentation increases. If the client is using retinoids and alpha hydroxy acids, they will experience a deeper peel. If hypopigmentation occurs, repigmentation of the peeled skin may take two to three months to regain its normal color.
Erythema
Persistent erythema is where the skin will become erythematous and appear quite red in the first few days following the peel. This erythema normally subsides gradually after the peel and should be completely resolved in two or three days.
Scarring
Scarring is the rarest, but most catastrophic, complication of deep peeling. Rare instances of scarring have been reported and, fortunately, are generally minor and can be treated successfully with topical steroids applied twice daily for one week. If treated at the first sign of prolonged erythema, the potential scar subsides after a few months.
Herpes Simplex
A herpetic breakout can be triggered by peeling in clients with or without a positive history for herpes. The eruptions will usually start on the lip or above the vermilion border. Since the peeling skin does not have a well-developed epidermis, it is not capable of forming a vesicle. Therefore, herpetic infections present as erosions rather than vesicles. The first sign of a herpetic lesion is pain. A client with a positive history of herpes viral infections should be treated 24 hours prior to the peel with 400 milligrams of oral acyclovir (Zovirax) three times a day for five days after the peel.
Infection
Infection is very rare, but may occur with superficial contamination of an open peeled area. Most clients never develop a true infection. If a peeled area becomes inflamed or infected, it can be treated with conventional antibiotics. Because infections commonly lead to scarring, any suspicion of infection should be treated aggressively. The organisms associated with peels are common bacterial pathogens, like staphylococcus, streptococcus, herpes simplex, and candida.
Milia and Acne
Milia and acne eruptions occasionally occur after a medium or deep peel as a consequence of follicular occlusion from the emollients and ointments used during the healing process. These small superficial cysts may appear at any time during the first week post-peel. In most cases, the milia-like cysts last a few days, but some can last several weeks and it may be necessary to manually remove them.
Allergic Reactions
Allergic reactions to chemical peels are very rare, although resorcinol does have the highest incidence of contact allergies. The problem with allergic reactions is that they can be difficult to diagnose because clients often already have erythema and edema associated with the peel. Signs of an allergic reaction may include hives appearing on the body, a constriction in the throat and difficulty breathing, or severe itching for hours after the peel.
Sun Sensitivity
Sensitivity to sunlight after a peel is increased, so sunscreen should be worn every day for protection from ultraviolet light exposure. An SPF of 15 to 30 is recommended and needs to be applied 30 minutes before going outside. Makeup formulated with SPF does not provide enough protection, however, some high-quality mineral makeups are natural ultraviolet reflectors and work well to protect the skin.
Emotional Responses
A pre-peel consultation and skin conditioning treatments are critical to building trust and properly educating clients on the benefits and possible side effects of exfoliating peels. In the case of a complication, loss of confidence on the part of the client can be very serious if they decide to file a lawsuit against the professional and their business. An informed consent should always be obtained and safety precautions should be followed. Clients with psychiatric illness or unrealistic expectations should not be treated with any level of chemical peel solution because the procedure may trigger a traumatic emotional response.
There are a wide range of peel solutions available that professionals can safely perform to achieve excellent results for ethnic skin. The potential for complications is a risk with all peels and methods of exfoliation in all skin types, especially for skin of color. Safe administration of a peel without complications is dependent on preparation, understanding peel depth and wound healing, post-peel homecare, and, most importantly, getting to know the client's skin before graduating from very superficial exfoliation to higher levels of peel intensity.
 Lyn Ross is a licensed master aesthetics instructor, accredited through the Georgia Board of Cosmetology with over 30 years of experience in the field of professional aesthetics. A true medical spa pioneer, Ross has written numerous articles, co-authored textbooks, and appeared on radio and television shows, highlighting professional aesthetics. She is dedicated to sharing her passion, knowledge, and years of clinical aesthetic experience. Ross provides skin care professionals with clinical and medical treatment protocols, products, and the education that guarantees client results and spa business success.
Lyn Ross is a licensed master aesthetics instructor, accredited through the Georgia Board of Cosmetology with over 30 years of experience in the field of professional aesthetics. A true medical spa pioneer, Ross has written numerous articles, co-authored textbooks, and appeared on radio and television shows, highlighting professional aesthetics. She is dedicated to sharing her passion, knowledge, and years of clinical aesthetic experience. Ross provides skin care professionals with clinical and medical treatment protocols, products, and the education that guarantees client results and spa business success.
Want to read more?
Subscribe to one of our monthly plans to continue reading this article.