For example, skin color is under exquisite hormone control.3 Only recently was it understood that the skin is a major producer of sex hormones, as well as many other types of hormones. All hormones require a specific type of receptor to be active. Due to the nature of these receptors and how they function, this article will discuss how hormones affect melanin production and acne vulgaris in relation to skin color in various ethnic groups.
Introduction to Hormone Receptors
Hormones must bind and interact with high-affinity receptors in order to have a biological effect in the skin. Within the human skin, there are receptors for peptide hormones and neurotransmitters. Most of these are water-soluble and unable to penetrate the lipid cell membrane; therefore, they appear on the cell surface. There is second group of receptors within the cell. This group includes steroid and thyroid hormones. These hormones are lipid soluble and can, therefore, bypass the cell membrane, travel through the cytoplasm, and interact with the nucleus. (See Figure 1.)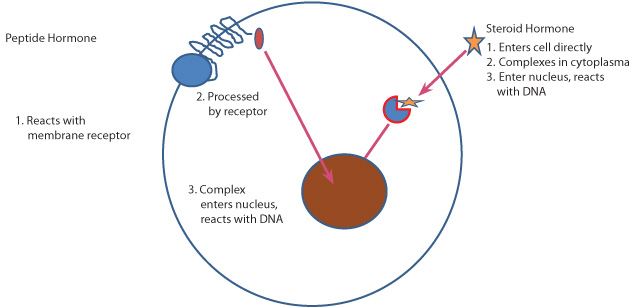
There are seven transmembrane domain receptors in human skin. These peptide hormone and neurotransmitter receptors contain an amino terminal extracellular domain, followed by seven hydrophobic amino acid segments, each of which spans the membrane bilayer. The last, or seventh segment, is followed by a hydrophilic carboxyl terminal domain, found within the cytoplasmic compartment. The box lists a number of hormone receptors which belong to this group. (See Figure 2.)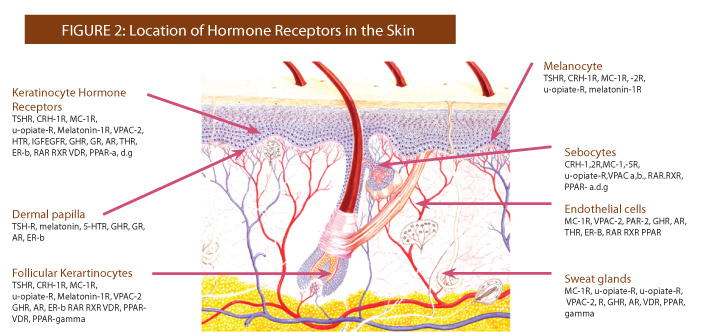
The second group of peptide receptors includes insulin/insulin-like growth factor I (IGF-I) receptor and the epidermal growth factor (EGF) receptor. These receptors are found in epidermal keratinocytes. Unlike the seven transmembrane-type receptors, these are single-transmembrane domain receptors.
The third group, which is similar to the second group, is represented by the growth hormone (GH) receptor. These receptors are present in many cell types,
including melanocytes and dermal fibroblasts, both epidermal and follicular keratinocytes of the outer root sheath, sebocytes, and cells of the sweat gland secretory duct. In addition, they are also found in hair matrix cells of the dermal papillae, endothelial cells, Schwann cells of peripheral nerves, and adipocytes of the dermis.
Steroid and Thyroid Hormones
These hormone receptors are classified as nuclear receptors. They differ from the receptors of the cell membrane in that they are transcriptional, meaning they utilize DNA transcriptional mechanisms to promote their biological effects. These hormone receptors operate within the nuclear chromatin to initiate the signaling cascade. These receptors in human skin can be grouped into two major subtypes based on shared structural and
functional properties.
The first group, the steroid receptor family, includes:
- The glucocorticoid receptor – found in basal keratinocytes, Langerhans cells and dermal fibroblasts.
- The androgen receptor (AR) – found in epidermal and follicular keratinocytes, sebocytes, sweat gland cells, dermal papilla cells, dermal fibroblasts, endothelial cells and genital melanocytes.
- The progesterone receptor – found only in basal epidermal keratinocytes.
The second group, the thyroid receptor family, includes:
- The thyroid hormone receptors – found in epidermal keratinocytes and dermal fibroblasts.
- The estrogen receptors – the β-form expressed in the skin, is detected in many cells of the skin, including epidermal and outer root sheath keratinocytes, melanocytes, dermal fibroblasts, dermal papilla cells, sebocytes, endothelial cells and adipocytes.
- The retinoic acid receptors – (RAR; isotypes α and γ) – and retinoid X receptors – (RXR; isotypes α, β, γ) – found in epidermal keratinocytes of the stratum granulosum, follicular keratinocytes, sebocytes and endothelial cells. Only the RXRα isotype is present in melanocytes, fibroblasts and inflammatory cells.
- The vitamin D receptor (VDR) – found in keratinocytes of all epidermal layers except those of the stratum corneum. It is found in epithelial cells of the epidermal appendages, melanocytes, Langerhans cells, CD11b macrophages and CD3 T-lymphocytes.
- The peroxisome proliferator-related receptors (PPAR) – found in epidermal and follicular keratinocytes, sebocytes, sweat gland cells, endothelial cells and adipocytes. Isotypes α and δ are also found in keratinocytes and sebocytes. Peroxisome prolifrator-related receptors δ are the predominant peroxisome proliferator-related receptor subtype in human keratinocytes, particularly in basal cells and suprabasal cells.
Hormonal Elements in Ethnic Skin Color
Variations in skin color appear to be a relatively recent development within humans, possibly 50,000 years ago. The presence of ultraviolet light is considered the main factor that determines skin color, since there is a gradation and the intensity of color from the tropics to the North Pole.4 It appears that females are generally lighter than males. This is due to their need for increased calcium during pregnancy. The light skin of the Scandinavians is an example of this phenomenon. While darker skin color is primarily a function of the amount of melanin in the skin per unit area, light skin color is more related to connective tissue, blood flow and light scattering than it is to pigment.5
Variations in skin color occur due to several factors including: genetics and melanin, the major pigment that determines skin color and protects the body from ultraviolet light. The inheritance of skin color is not a simple process. It is the result of several complex processes including: melanogenesis and many of the factors which influence the development of melanin, including hormones.
Heredity in Skin Color Genes
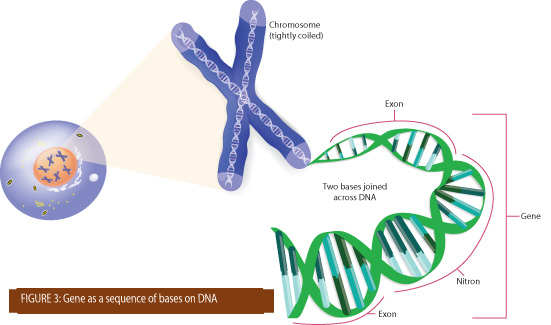
Let’s start with the basics. “A gene is the molecular unit of heredity of a living organism. It is widely accepted by the scientific community as a name given to some stretches of deoxyribonucleic acids (DNA) and ribonucleic acids (RNA) that code for a polypeptide or for an ribonucleic acids chain that has a function in the organism, though there still are controversies about what plays the role of the genetic material.”6 DNA is a complex chain that makes up the chromosomes. Chromosomes contain specific segments known as genes. (See Figure 3.) There are three genes which we will discuss that are responsible for skin color. The first is melanocortin 1 receptor (MC1R) gene, which is responsible for selecting the production of either pheomelanin or eumelanin. Light skin appears to have evolved along a different genetic pathway and two genes appear responsible for this phenomenon. The first is known as KIT Ligand (KITLG), and the second is known as Agouti Signaling Peptide (ASIP). These are the major pigment associated genes which we shall cover. The genes responsible for skin pigment are also complex; in fact, they are alleles. “An allele, or allel, is one of a number of alternative forms of the same gene or same genetic locus (generally a group of genes). It is the alternative form of a gene for a characteristic, producing different effects. Sometimes different alleles can result in different observable phenotypic7 traits, such as different pigmentation.”8 Cutaneous pigmentation is under complex genetic control regulated by more than 150 alleles spread over 90 loci. Protein products of these loci acting as enzymes, structural proteins, transcriptional regulators, transporters, receptors, and growth factors, have a wide array of functions and cellular targets. Skin color is partly related to genetics and partly related to environmental factors. There are usually two genes inherited for each trait, one from the father and one from the mother. For example, eye color is an extremely complicated genetic process. Many genes, as many as 15 or more, are believed to be involved in eye color.9
Melanin is produced by melanocytes in a process called melanogenesis, within small membrane–bound packages called melanosomes, which are transferred to the keratinocytes. The main purpose of the melanosomes is to protect the keratinocytes from ultraviolet damage. The differences in skin colors are due to the melanocytes producing different amounts and different types of melanin. The main genetic process underlying human skin color is the enzyme tyrosinase, which is responsible for the color of the skin, eyes, and variation in hair shades.
There are two types of melanin: eumelanin, a brown-black polymer of dihydroxyindole carboxylic acids, is found in hair, areola, and skin, and the hair colors grey, black, yellow, and brown. The second type, known as pheomelanin, has a pink-to-red hue and is found in large quantities in red hair, the lips, nipples, glans of the penis, and vagina.
The amount and type of melanin produced is controlled by a number of genes that operate under incomplete dominance. It appears that dark skin evolved about 1.2 million years ago, about the same time that humans lost their body hair.10
 Effect of Hormones on Skin Color
Effect of Hormones on Skin Color
The genetic control of skin color is based on a combination of specific hormones and specific receptors in the skin. The major receptor for the production of melanin is the melanocortin1 receptor (MC1R), of which there are five types. There are three major melanocyte-stimulating hormones that are produced by cells in the intermediate lobe of the pituitary gland. Melanocyte-stimulating hormone (MSH) belongs to a group called the melanocortins. This group includes alpha-melanocyte-stimulating hormone (α-MSH), beta-melanocyte-stimulating hormone (β-MSH) and gamma-melanocyte-stimulating hormone (γ-MSH); these peptides hormones are formed from a large precursor peptide called pro-opiomelanocortin (POMC). Of these, the most important for pigmentation is α-MSH. In addition to stimulating melanocytes to produce melanin, α-MSH provides the switch from the production of eumelanin to pheomelanin and back again. This can occur in the same melanocyte; however, each melanocyte can only make one type of melanin at a time.
Both melanocyte-stimulating hormone and α-MSH are capable of stimulating melanin production in sun exposed areas under the action of ultraviolet light. Prolonged dosages of α-MSH, however, will not only increase pigmentation of the skin, but may also cause hypertrichosis (excessive hair growth) and skin atrophy. Changes in the melanocortin1 receptor, particularly mutations which reduce their receptivity to melanocyte-stimulating hormones, are often associated with light skin or red hair.11 It is the variations of the melanocortin1
receptor present in the white population that accounts for the red hair phenotype and fair skin, as well as the decreased ability to tan, in approximately 50 percent of the people in this group.
Disorders of Pigmentation – Estrogens and Androgens
Overproduction of melanin results in what is known as hyperpigmentation while underproduction results in hypopigmentation. Two hormones that contribute prominently in these disorders are estrogen and androgens. Individuals who have elevated estrogen levels tend to develop a type of hyperpigmentation known as melasma. The effects of estrogen on melanogenesis are uncertain; however, it is believed that the effects of estradiol on tyrosinase activity are influenced by many factors, including both sex and age. Estrogens affect skin thickness, wrinkle formation, and skin moisture. Estrogens increase glycosaminoglycans (GAGs) and increase collagen production. Skin pigmentation is increased in certain sun-exposed areas as the forehead, nose, and cheeks, producing a condition known as melasma.
Melasma is a true hormonal-induced pigment disorder; one that is poorly understood. The number of melanocytes in those areas is not increased, but the melanocytes are larger, more dendritic, and show increased melanogenesis of eumelanin. In the third trimester of pregnancy, elevated levels of estrogen, progesterone, and melanocyte-stimulating hormones contribute to melasma.12 The skin is not the only external feature that benefits from estrogens. Hair growth is influenced considerably by estrogen as is evident in the luxuriant hair growth experienced in pregnancy. On the other hand, estrogens are also capable of causing thinning hair, a condition which, when severe, is known as telogen effluvium.13
Androgens are secreted primarily by the adrenal glands and the gonads and express their activity through the androgen receptor (AR), on the melanocyte. The skin is a major target for androgens as the androgen receptor is found in the epidermis, the dermis, sebaceous gland, and hair follicle. It is interesting to note that individuals with low testosterone, such as white eunuchs, do not respond to ultraviolet light. Skin is subject to increased pigmentation after puberty and during pregnancy. Vitiligo, the most common type of hypopigmentation, may improve with the oral administration of a combination of testosterone and estrogen.14 In vitiligo, the defect appears to relate to some damage or destruction of the melanocyte, making it incapable of melanin production. Androgens modulate tyrosinase activity through regulation of cAMP, a key regulator of skin pigmentation.
Details of the mechanisms by which sex hormones influence melanogenesis remain elusive. There is evidence of concurrent involvement of different cellular factors (secondary messengers, growth factors, et cetera) in multiple molecular pathways within the skin, eliciting hyperpigmentation. There is no question that estrogen affects pigmentation during pregnancy and that certain birth control pills can also increase skin pigmentation.15 We know that there are multiple receptors on the melanocytes for both estrogen and androgens, but we are not certain exactly how they increase melanogenesis.
Vitamin D and Skin
Vitamin D is made from cholesterol in the skin when stimulated ultraviolet light. The cholesterol is converted to previtamin D3, and then to 1, 25
dihydroxy-cholecalciferol in the kidney and in the liver. Proliferation of melanoma cells is inhibited by 1, 25 dihydroxy-cholecalciferol, though not all melanoma cells will express the vitamin D receptor, or are responsive to vitamin D. Certain types of vitamin D receptors may be associated with red hair. (Some melanoma patients and hyperpigmentation may occur when vitamin D is applied to these as in the case of psoriasis.)
Post-inflammatory Hyperpigmentation
Post-inflammatory hyperpigmentation appears as hyperpigmented macules with a rather indistinct feathery edge and may involve both the epidermis and dermis. They appear after resolution of inflammatory skin lesions like acne, contact dermatitis, or atopic dermatitis. Post-inflammatory hyperpigmentation is more common in patients with darker skin and is characterized histologically by a normal number of melanocytes, but with increased melanin production. Like ultraviolet exposure, post-inflammatory hyperpigmentation occurs after the event in the healing phase. While not directly related to sex hormones, it is believed it is part of the arachidonic acid cascade and involves leukotrienes, particularly LTC4 and LTD4. Not a great deal is known in this area, but there appears to be a considerable amount of research going on at this time.16
Ethnic Variations in Acne
The biggest problem in treating acne in people of color is the prevention of hyperpigmentation. There are approximately 2,000 epidermal melanocytes per square millimeter on the head and forearms, and 1,000 epidermal melanocytes per square millimeter on the rest of the body. People of color are most concerned about preventing any inflammation or injury to the skin that can produce hyperpigmentation. Unfortunately, almost any inflammatory process can initiate a hyperpigmentation process. Acne vulgaris is one of the most common dermatological diseases, with 40 to 50 million individuals in the United States affected with acne.17 Often defined as people of color – African Americans, Asians, that Latinos, and Arabs – all have approximately the same incidence of acne.18 Acne in skin of color appears to develop by the same pathogenesis that occurs in Caucasian patients. The controversy over whether differences exist in certain biological characteristics of skin, such as sebum production and bacterial content, among various racial/ethnic groups continues.19 Studies published evaluating racial/ethnic differences in sebaceous gland size and activity compared to Caucasian skin have not been confirmed. A recent study evaluated 18 African American and 19 Caucasian patients for differences in certain skin surface properties, such as sebum level, pH, moisture content, and barrier function, discovered no significant differences in sebum production between African American and Caucasian patients.20 However, transepidermal water loss (TEWL) measurements show that African Americans and Caucasians were significantly different (p Northern Asian > African American, indicating a better barrier function for African Americans. African American women had more total lipid production than Northern Asian or Caucasian women. Three lipid classes (free fatty acids, triglycerides and wax esters) were analyzed and showed that the trend became significant (p 0.05) in the wax ester fraction when directly comparing African Americans with Caucasians. Additionally, six lipids were identified in the wax ester fractions that were significantly different in quantity (p 0.05) between African Americans and Caucasians.21 These results identified significant differences in sebaceous lipid profiles across ethnic groups and determined that the differences correlated with skin barrier function. How this relates to the genesis of acne is not known, but a recent study does indicate a biochemical difference between ethnic skin types. An elevated level of TGF-β1 present from dermal fibroblasts derived from African American skins correlated with the higher levels of TGF-β mRNA in African American skins analyzed by cDNA array (a molecular biochemical technique). Treatment with TGF-resulted in a considerable difference in the elastin content between the African American skin and the Caucasian skin, the level being higher in African American skin.22
Summary
Hormones have physiological effects on skin, particularly in the formation of collagen, elastin and glycosaminoglycans. The effect of estrogen and testosterone on acne is also well-established. Thyroid hormone also has a profound effect on skin and hair growth. The adrenal glands are associated with pigmentation in both Addison’s disease and Cushing’s disease, but independent of these two disorders, they also have a profound effect on skin and muscle. It would take two very large textbooks to cover all the effect of hormones on normal body physiology, and an additional one just to cover the effect of hormones on skin. An excellent reference book on hormones is by Griffin Strauss and Strauss.23 If we are to discover any real difference between the biochemistry and microanatomy among ethnic groups, there is still much work to be done. Since most of the disorders that affect skin are fairly uniform across the ethnic types, it would appear that the differences between the various races is minor and not of major importance. However, the subtle differences that we are finding indicate further research should be pursued.
References
1 Zouboulis, Christos C. 2000. “Human skin: An independent peripheral endocrine organ”. Horm Res 54: 230-242.
2 Orfanos, C. E., R. Happle, and F.J.G. Ebling. 1990. “Chapter 12: The Hormonal Control of Hair Growth.” Hair and hair diseases. Berlin: Springer-Verlag.
3 Suzuki I., Cone R.D., Im S., Nordlund J., Abdel-Malek ZA. 1996. “Binding of melanocortin hormones to the melanocortin receptor MC1R on human melanocytes stimulates proliferation and melanogenesis”. Endocrinology 137: 1627-1633.
4 Muehlenbein, Michael. 2006.“Human Evolutionary Biology”. Cambridge University Press. pp. 192–213. 2010.
5 Jablonski, N.G. Skin: a Natural History. Berkeley: University of California Press.
6 Pearson, H. 2006. “Genetics: what is a gene?”. Nature 441 (7092): 398–401.
7 The phenotype is the end result of the action of a gene, red hair, for example is the phenotype and the genotype is the genetic code for pheomelanin.
8 Malats N, Calafell F. July 2003. “Basic glossary on genetic epidemiology”. Journal of Epidemiology and Community Health 57 (7): 480–2.
9 Mason, Clyde W. 1924. “Blue Eyes”. Journal of Physical Chemistry 28 (5): 498–501.
10 Rogers, Alan R.; Iltis, David; Wooding, Stephen. 2004. “Genetic Variation at the MC1R Locus and the Time since Loss of Human Body Hair”. Current Anthropology 45: 105–8.
11 Schaffer J.V. and Bolognia J.L. “The melanocortin-1 receptor: red hair and beyond”. Arch Dermatol 137: 1477–1485, 2001.
12 McLeod, S. D., Ranson, M., Mason, R. S. 1994. “Effects of estrogens in human melanocytes in vitro”. J. Steroid Biochem. Mol. Biol. 49,9-14
13 Verdier-Sévrain, S., et al. 2006. “Biology of estrogens in skin: implications for skin aging”. Experimental Dermatology, 15: 83–94.
14 Muto M, Furumoto H, Ohmura A, and Asagami C. 1995. “Successful treatment of vitiligo with a sex steroid-thyroid hormone mixture”. J Dermatol 22: 770–772.
15 Tadokoro, T., Rouzaud, F., Itami, S., Hearing, V. J., Yoshikawa, K. 2003. “The inhibitory effect of androgen and sex-hormone-binding globulin on the intracellular cAMP level and tyrosinase activity of normal human melanocytes”. Pigment Cell Res. 16,190-197.
16 Pentland, A. P., Mahoney, M. G. 1990. “Keratinocyte prostaglandin synthesis is enhanced by IL-1”. J. Invest. Dermatol. 94,43-46.
17 White, G.M. 1998. “Recent findings in the epidemiologic evidence, classification, and subtypes of acne vulgaris”. J Am Acad Dermatol. 39:S34–S37.
18 Alexis, A.F., Sergay, A.B., and Taylor, S.C. 2007. “Common dermatologic disorders in skin of color: a comparative practice survey”. Cutis. 80:38–394.
19 Kligman, A.M. and Shelley, W.B. 1958. An investigation of the biology of the sebaceous gland. J Invest Dermatol. 30:99–125.
20 Grimes P., Edison, B.L., Green, B.A., et al. 2004. “Evaluation of inherent differences between African American and white skin surface properties using subjective and objective measures”. Cutis. 73:392–396.
21 Diridollou S., de Rigal J., Querleux B., Leroy F., and Holloway Barbosa V. 2007. “Comparative study of the hydration of the stratum corneum between four ethnic groups: influence of age. Int J Dermatol”. 46(Suppl 1):11–4.
22 Fantasia J., Lin C.B., Wiwi C., Kaur S., Hu Y.P., Zhang J., and Southall M.D. June 2013. “Differential levels of elastin fibers and TGF-β signaling in the skin of Caucasians and African Americans”. J Dermatol Sci. 70(3):159-65. Griffin JE, 24.
24 Stauss, D. and Strauss, R.C. April 8, 2004. RC Textbook of Endocrine Physiology, Oxford University Press.
 Michael Q. Pugliese, BS, L.E. became the third generation CEO of Circadia by Dr. Pugliese, Inc. in 2006. Under his leadership, the Circadia brand has grown to achieve international recognition and distribution. Pugliese is a member of the Society of Cosmetic Chemists and regularly attends their education events to stay on the cutting edge of new product development. His compelling original lectures honor the tenets of modern skin science discovered by his grandfather, and add today’s application of that information in an ever-changing business and scientific environment.
Michael Q. Pugliese, BS, L.E. became the third generation CEO of Circadia by Dr. Pugliese, Inc. in 2006. Under his leadership, the Circadia brand has grown to achieve international recognition and distribution. Pugliese is a member of the Society of Cosmetic Chemists and regularly attends their education events to stay on the cutting edge of new product development. His compelling original lectures honor the tenets of modern skin science discovered by his grandfather, and add today’s application of that information in an ever-changing business and scientific environment.
 Peter T. Pugliese, M.D. has been a pioneer of cosmetic research, formulation and education in the field of skin health. He has spent over 50 years dedicating his life to research and science. His research in the field of anti-aging and skin physiology has given him numerous awards, patent, and discoveries which have influenced the course of professional skin care. He has authored four books, including the first textbook written for aestheticians by a physician, Advanced Professional Skin Care, to bridge aesthetics and medicine with a common language. His newest publication is Advanced Professional Skin Care – Medical Edition.
Peter T. Pugliese, M.D. has been a pioneer of cosmetic research, formulation and education in the field of skin health. He has spent over 50 years dedicating his life to research and science. His research in the field of anti-aging and skin physiology has given him numerous awards, patent, and discoveries which have influenced the course of professional skin care. He has authored four books, including the first textbook written for aestheticians by a physician, Advanced Professional Skin Care, to bridge aesthetics and medicine with a common language. His newest publication is Advanced Professional Skin Care – Medical Edition.